


Mental health billing trips up more practices than almost any other specialty. The documentation standards are stricter, payer rules are less predictable, and denial rates run higher than in general medical billing.
A single missed authorization or one mismatched code can mean weeks of delayed payment or a flat-out rejection.
This guide walks through everything a mental health practice needs to submit clean claims, reduce denials, and get paid consistently.
It covers the full billing workflow from intake through payment posting, the CPT codes used most often, insurance verification, compliance requirements, and the decision of whether to handle billing in-house or outsource it.
Whether you run a solo therapy practice, a group counseling center, or a psychiatric facility, the fundamentals covered here apply directly to your revenue cycle.
What Mental Health Claims Submission Actually Involves
Mental health claims submission is the process of sending billing data to an insurance company after a covered service is rendered.
The claim communicates who the patient is, what diagnosis was treated, what procedure was performed, who provided it, and when. The payer reviews that information and either pays, denies, or requests additional documentation.
On the surface it sounds straightforward. In practice, behavioral health billing adds layers that other specialties rarely deal with:
- Sessions are timed, and the wrong code for the wrong duration gets rejected
- Prior authorization is frequently required before treatment even starts
- Many insurers carve out mental health benefits to a separate administrator
- Documentation standards are scrutinized harder than in most medical fields
- Denial rates in behavioral health run significantly above the national average
Understanding these realities upfront is what separates practices that get paid consistently from those that spend weeks chasing claims.
The Full Mental Health Claims Submission Workflow
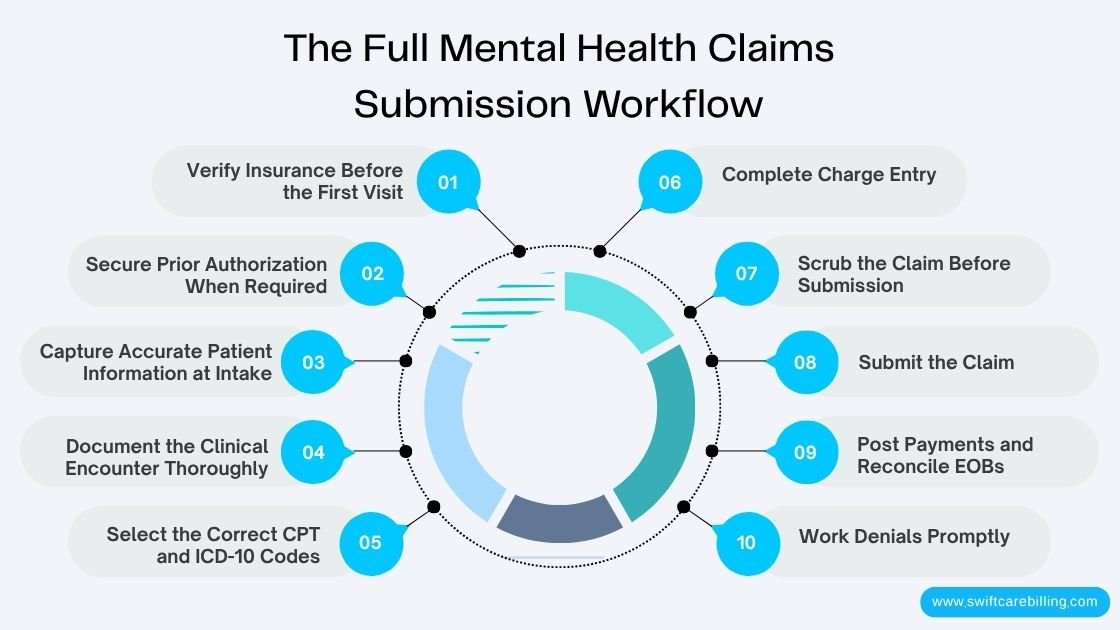
Clean claims start with a clean process. Every step below has a direct impact on whether a claim gets paid on the first submission.
Step 1: Verify Insurance Before the First Visit
Nothing downstream matters if the coverage verification is wrong. Before any session takes place, confirm the following with the insurer:
- Is the policy active on the date of service?
- Does the plan include outpatient mental health benefits?
- Is the patient’s mental health coverage managed by a separate carve-out company?
- What is the copay, deductible, and coinsurance for behavioral health visits?
- Is there a session limit per calendar year?
- Is prior authorization required, and for which services?
Call the provider services line directly. Do not rely on the patient’s description of their own coverage. Mental health benefits, in particular, are often misunderstood by policyholders. Record what you’re told, who you spoke with, and the reference number.
Step 2: Secure Prior Authorization When Required
Many payers require approval before mental health services begin, especially for anything beyond a handful of initial visits. Services that most commonly require authorization include:
- Ongoing outpatient therapy beyond session limits
- Intensive outpatient programs (IOP)
- Partial hospitalization programs (PHP)
- Psychological and neuropsychological testing
- Residential treatment
Submit the authorization request before the patient’s first appointment whenever possible. If authorization is denied or expires mid-treatment, document the appeal promptly. Providing services without authorization almost always results in a non-payment.
Step 3: Capture Accurate Patient Information at Intake
Every claim rejection trace back to data. At intake, collect and confirm:
- Full legal name exactly as it appears on the insurance card
- Date of birth
- Subscriber ID, including any letters or dashes
- Group number
- Relationship to policyholder if the patient is a dependent
- Current mailing address
A name that does not match the insurer’s records will trigger an automatic rejection. Take time at intake to verify the card against the patient’s ID.
Step 4: Document the Clinical Encounter Thoroughly
Clinical documentation is the single most audited aspect of mental health billing. Payers look for evidence that the service was medically necessary and that the code billed reflects what actually happened. Every session note must include:
- Date of service
- Session start and end times
- Location or place of service
- Clinician’s credentials and signature
- Diagnosis and how it connects to the treatment being provided
- Specific interventions used during the session
- The patient’s response to treatment
- Progress toward goals outlined in the treatment plan
- Plan for the next session
Vague notes are one of the most common reasons mental health claims face post-payment audits and clawbacks. If the documentation does not justify the service, the reimbursement is at risk even after it has been received.
Step 5: Select the Correct CPT and ICD-10 Codes
Coding accuracy determines whether a claim pays or gets rejected. Mental health uses a specific set of procedure codes, most of which are time-based. The diagnosis code must support the procedure, and both must align with what the clinical notes describe.
See the full CPT code section below for detailed guidance.
Step 6: Complete Charge Entry
Once codes are confirmed, enter the billing data into your practice management system or billing software. This includes:
- CPT codes
- ICD-10 diagnosis codes
- Modifiers if applicable
- Units
- Fee schedule charges
- Place of service code
Every field must match the documentation. Discrepancies between the chart and the claim create denial risk even when the underlying service is unquestionable.
Step 7: Scrub the Claim Before Submission
Running claims through a scrubber before submission catches errors that would otherwise result in a rejection. Good claim scrubbing software flags:
- Missing or invalid NPI numbers
- Invalid or mismatched diagnosis codes
- Incorrect place of service for the billed service
- Missing authorization numbers
- Code combinations that payers do not allow
- Duplicate claims for the same date of service
The time spent scrubbing is a fraction of the time it takes to fix and resubmit a denied claim.
Step 8: Submit the Claim
Electronic submission through a clearinghouse is the standard for professional claims. It’s faster, produces a confirmation receipt, and allows for tracking. Paper claims are slower, generate more rejections, and should only be used when a payer requires them.
For individual providers and group practices billing professional services, the CMS-1500 form is the standard. Facilities use the UB-04. Most clearinghouses accept 837P (professional) and 837I (institutional) file formats.
Most payers require claims within 90 to 180 days of the date of service. Know your payer-specific timely filing windows and build submission deadlines into your workflow.
Step 9: Post Payments and Reconcile EOBs
When a payment arrives, post it accurately and reconcile against the Explanation of Benefits (EOB) or remittance advice. Compare what was paid against your fee schedule and contracted rates. If the payer has underpaid, address it before closing the claim.
Payment posting also reveals patterns. If the same payer is consistently underpaying on a specific CPT code, that is worth investigating and potentially appealing.
Step 10: Work Denials Promptly
Denials do not resolve themselves. The moment a denial comes in, identify the reason code from the EOB and determine whether the issue is correctable. Common denial reasons and their remedies:
- Missing authorization — Obtain retro authorization if possible, then appeal
- Incorrect CPT code — Correct and resubmit with a corrected claim
- Insufficient documentation — Attach clinical notes and appeal
- Eligibility issue — Verify coverage for the date of service, correct, and resubmit
- Timely filing exceeded — Submit with proof of timely filing if available
Most payers give you between 60 and 180 days to appeal a denial. Track deadlines the same way you track submission deadlines.
Mental Health CPT Codes: What Each One Covers
Getting the right code on the right claim is not guesswork. Each code has specific criteria. The most common mental health CPT codes and their rules are below.
Individual Psychotherapy (90832, 90834, 90837)
These three codes cover the majority of individual therapy sessions. The key differentiator is time. The session duration in your clinical notes must support whichever code you select.
- 90832 — Psychotherapy, 16 to 37 minutes
- 90834 — Psychotherapy, 38 to 52 minutes
- 90837 — Psychotherapy, 53 minutes or more
Document the exact start and end time of the session. Using 90837 for a 45-minute session is an overcoding error that creates audit risk. Using 90832 for a 60-minute session is an undercoding error that costs the practice revenue.
Psychiatric Diagnostic Evaluation (90791)
Use 90791 for the initial assessment with a new patient. This code covers a comprehensive evaluation that includes history-taking, mental status examination, diagnosis formulation, and treatment planning. It is a one-time code per patient relationship — it is not appropriate for ongoing therapy visits.
Some payers require authorization for the diagnostic evaluation itself. Verify before the first appointment.
Group Psychotherapy (90853)
90853 is billed once per patient, per session, regardless of how many people are in the group. The session must be led by a qualified provider and must involve therapeutic group interaction, not just a structured class or education session. Document attendance, the nature of the group intervention, and each patient’s participation and response.
Family Therapy (90846, 90847)
Family therapy codes are used when the patient’s diagnosed condition is the focus and family participation is part of the treatment plan:
- 90846 — Family or couples therapy without the patient present
- 90847 — Family or couples therapy with the patient present
These codes are not appropriate for general family counseling unrelated to a patient’s mental health diagnosis. The clinical notes must connect the family session directly to the patient’s treatment goals.
Interactive Complexity Add-On (90785)
90785 is an add-on code used when specific factors make a session significantly more difficult. Qualifying factors include the presence of a translator, a legally authorized representative, a disruptive third party, or a patient whose communication is severely impaired. This code must always be billed with a primary service like 90791 or 90837. It cannot stand alone.
Evaluation and Management with Psychotherapy
When a prescribing clinician provides both medication management (an E/M service) and psychotherapy in the same visit, both can be billed together. The documentation must clearly distinguish the time and work involved in each service. The two portions of the visit must be separate and significant. The psychotherapy add-on codes (90833, 90836, 90838) are used alongside the E/M code to reflect the combined visit.
Telehealth Billing for Mental Health
Telehealth mental health services are billed using the same CPT codes as in-person visits. The difference is in the modifier and place of service code. For most payers:
- Place of Service 02 — Telehealth provided other than in patient’s home
- Place of Service 10 — Telehealth provided in patient’s home
- Modifier GT — Via interactive audio and video telecommunication systems
- Modifier 95 — Synchronous telemedicine service rendered via real-time interactive audio and video
Telehealth rules vary by payer. Medicare, Medicaid, and commercial plans each have their own policies on eligible services, provider types, and state requirements. Verify telehealth coverage separately during benefits verification.
Common ICD-10 Codes in Mental Health Billing
The diagnosis code must support the service billed. Below are frequently used ICD-10 codes in behavioral health:
- F32.1 — Major depressive disorder, single episode, moderate
- F33.0 — Major depressive disorder, recurrent, mild
- F41.1 — Generalized anxiety disorder
- F41.0 — Panic disorder
- F43.10 — Post-traumatic stress disorder, unspecified
- F43.12 — PTSD, chronic
- F90.0 — ADHD, predominantly inattentive presentation
- F31.9 — Bipolar disorder, unspecified
- F20.9 — Schizophrenia, unspecified
- F10.10 — Alcohol use disorder, mild
Use the most specific code available. General or unspecified codes increase scrutiny from payers and may trigger additional documentation requests.
How to Verify Insurance Coverage for Mental Health Patients
Insurance verification is the front line of mental health billing. When it is done right, most claim problems are prevented before they start. When it is skipped or done sloppily, denials are almost inevitable.
Call the Provider Line, Not the Member Line
Always call the provider services number on the back of the insurance card, not the member services number. The provider line gives more detailed benefit information and documents the call under your NPI. Have the following ready before you call:
- Your practice’s NPI number
- Your Tax ID
- Patient’s full name, date of birth, and subscriber ID
Ask specifically about outpatient mental health benefits. General medical coverage does not always include behavioral health, and the information from one department may not apply to the other.
Questions to Ask During Every Verification Call
- Is the patient’s mental health coverage managed by a separate company?
- Is the policy active on the anticipated date of service?
- Is the patient’s deductible met? If not, how much remains?
- What is the copay or coinsurance for outpatient mental health sessions?
- Is there an annual session limit for psychotherapy?
- Is prior authorization required for initial sessions? For ongoing sessions?
- Is your practice in-network with this plan?
- What is the correct mailing address or clearinghouse for claim submissions?
Document every answer, including the name of the representative and a reference number. If there is ever a dispute, this record supports your position.
Understand the Plan Type Before Assuming Coverage
HMO plans require patients to stay within a defined network. If your practice is not in-network with an HMO, the patient may have no coverage at all for your services. PPO plans give patients the option to go out-of-network, though at a higher cost. EPO plans operate like PPOs but without any out-of-network coverage. Knowing the plan type tells you immediately whether you need to address a potential coverage gap before treatment begins.
Handling Carve-Out Plans
Many large employers and insurers carve out behavioral health benefits to a separate managed care company. Optum, Magellan, and Beacon Health Options are common carve-out administrators. The patient’s medical insurance card may not reflect this. If you call the medical plan and they direct you to a behavioral health administrator, do not skip that second call. The carve-out company controls the authorization, the fee schedule, and the claim submission address.
Out-of-Network Patients
If you are out-of-network with a patient’s plan, the next step depends on the plan type. Ask whether there are any out-of-network mental health benefits. If so, confirm the reimbursement rate and whether the patient has a separate out-of-network deductible. Discuss the financial implications with the patient before the first session. Providing care and informing the patient of costs after the fact creates collection problems and erodes trust.
Why Mental Health Claims Get Denied and How to Fix Them
Mental health claims face higher denial rates than most other specialties. Understanding the most common denial reasons removes most of the guesswork from your A/R management.
Missing or Expired Authorization
This is the number one denial reason in behavioral health. If a payer requires prior authorization and the service is rendered without it, the claim will be denied. If an existing authorization expires mid-treatment, claims for services after the expiration date will also be denied. Build authorization tracking into your workflow. Know the expiration date, how many sessions are approved, and when to submit a request for continued care.
Incorrect or Mismatched Codes
A CPT code that does not match the documentation, a diagnosis code that does not support the procedure, or a code that the payer does not allow for that provider type — all of these produce denials. Review coding on every claim before submission, not after.
Insufficient Medical Necessity Documentation
Payers have the right to request medical records to verify that a service was necessary. If your documentation does not clearly establish the diagnosis, the functional impairments, and the rationale for treatment, the claim is vulnerable. Write notes that a reviewer who has never met the patient can read and understand as justification for every service billed.
Eligibility Issues
Coverage may have ended due to a lapse in premium payment, a change in employment, or an enrollment error. Always verify eligibility on or close to the date of service, not just at intake. A patient whose coverage was active at the start of treatment may not be covered three months later.
Timely Filing Violations
Claims submitted after a payer’s filing deadline are denied and typically cannot be appealed. Most payers have windows between 90 and 365 days from the date of service. Know your payer-specific limits and submit as soon as possible after each session.
Coordination of Benefits Errors
When a patient has more than one insurance policy, the primary payer must be identified and billed first. Billing the secondary payer before the primary processes the claim will result in a denial. Verify COB status during insurance verification and update it any time a patient reports a change.
Duplicate Claim Denials
Submitting the same claim twice — whether to fix an error or out of impatience — triggers an automatic duplicate denial on the second submission. Always submit a corrected claim with a corrected claim indicator, not a duplicate of the original.
Compliance and Regulatory Requirements in Mental Health Billing
Behavioral health billing operates under a stricter compliance environment than most specialties. Two layers of regulation apply: the standard HIPAA framework that governs all healthcare, and additional rules specific to mental health and substance use disorder treatment.
HIPAA Requirements
All protected health information (PHI) must be safeguarded at all times, including during billing operations. This means secure transmission of claims data, access controls on billing systems, and proper handling of paper documents. Mental health records are subject to the same HIPAA standards as general medical records, though providers often apply additional discretion due to the sensitive nature of behavioral health information.
42 CFR Part 2 for Substance Use Disorder Records
Substance use disorder treatment records are protected by federal regulations stricter than standard HIPAA rules. Records related to SUD treatment cannot be shared without specific written patient consent, even with other treating providers, in most circumstances. This affects what documentation can be submitted with a claim and what can be disclosed during an audit. Practices treating substance use disorders must maintain separate protocols for these records.
Medical Necessity Standards
Every service billed must be medically necessary. This means the treatment must be appropriate for the patient’s diagnosed condition, consistent with accepted standards of care, and not provided primarily for the convenience of the patient or provider. Clinical documentation must establish medical necessity for every claim. Payers that audit claims will deny services they determine were not medically necessary, and in cases of repeated issues, this can trigger a broader compliance review.
Mental Health Parity Laws
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires that health insurance plans covering mental health and substance use disorder benefits do so at parity with medical and surgical benefits. This means payers cannot impose stricter session limits, higher cost-sharing, or more burdensome authorization requirements for mental health services than they apply to comparable medical services. If a payer is denying claims in ways that appear inconsistent with parity requirements, that denial may be appealable on parity grounds.
Accurate Coding and Anti-Fraud Compliance
Upcoding — billing a higher-level service than what was provided — and unbundling — billing separately for services that should be combined — are both fraudulent billing practices. They expose the practice to overpayment demands, exclusion from insurance networks, and potential False Claims Act liability. Every code submitted should reflect exactly what the documentation supports. When in doubt, use the lower code and document more thoroughly next time.
Best Practices That Reduce Denials and Speed Up Payments
Standardize Your Documentation Templates
Therapists working from the same documentation template produce more consistent, billable notes than those writing from scratch each session. Build a template that prompts for all required elements: session times, diagnosis, intervention description, patient response, progress toward goals, and plan for next session. Consistency protects claims in audits and reduces the time spent writing notes.
Submit Claims Within 48 Hours of Service
The longer you wait to submit, the greater the risk. Build a workflow that gets claims submitted within 48 hours of the session date. For practices with high volume, daily batch submissions are more effective than weekly ones. Early submission also means earlier payment posting.
Track Every Claim Through to Payment
Submitting a claim is not the finish line. Follow up on unpaid claims at regular intervals — 14 days for electronic claims and 30 days for paper claims is a reasonable starting point. Use your practice management software or billing platform to flag claims that have not received a response within those windows.
Train Staff on Payer-Specific Rules
No two payers operate exactly the same way. Some require specific modifier combinations. Some have different timely filing windows. Some require authorization for initial evaluations while others do not. Build a payer-specific reference document for your most common insurance plans and update it regularly.
Appeal Denials Consistently
Many practices write off denied claims instead of appealing them. Most denials are correctable. For authorization-related denials, contact the payer and request a peer-to-peer review or submit a retro authorization request along with supporting clinical documentation. For coding denials, correct the claim and resubmit. Track appeal outcomes by denial type to measure whether your process is working.
Use Claim Scrubbing Consistently
Every practice should scrub every claim before submission. This is non-negotiable. A clean claim rate above 95% is achievable with disciplined pre-submission review. Every claim that fails scrubbing and gets caught before submission saves the time and money that would go into managing a denial.
Monitor Your Key Billing Metrics
Running a practice without measuring billing performance is like driving without gauges. Track the following metrics monthly:
- Clean claim rate — percentage of claims paid on first submission
- Denial rate by payer and code
- Days in accounts receivable
- Average reimbursement per CPT code
- Write-off rate by denial reason
Patterns in these numbers point directly to where the billing process is breaking down.
Should You Outsource Mental Health Billing?
Mental health billing is complex enough that many practices reach a point where managing it internally no longer makes financial sense. The right answer depends on the size of your practice, your current denial rate, and how much administrative time your clinical staff is spending on billing tasks.
The Real Cost of In-House Billing
In-house billing costs include salary and benefits for billing staff, practice management software, clearinghouse fees, training and continuing education, and the cost of claim errors that go undetected. Beyond direct costs, there is also the opportunity cost of clinical staff time spent on billing administration instead of patient care. When billing errors are frequent or denial follow-up is delayed, the revenue impact compounds over time.
What Outsourced Billing Delivers
A specialized medical billing company with experience in behavioral health brings a dedicated team of coders and billers who work mental health claims every day. For most practices, this translates to:
- Higher clean claim rates on the first submission
- Faster follow-up on unpaid and denied claims
- Consistent authorization tracking
- Access to billing software without the licensing cost
- Regular reporting on key revenue cycle metrics
Practices with denial rates above 10% or A/R days above 45 are usually good candidates for outsourcing. The improvement in collections often more than offsets the cost of the service.
What to Look for in a Mental Health Billing Partner
Not all billing companies have behavioral health expertise. When evaluating a partner, ask about:
- Experience specifically with mental health and substance use disorder billing
- Familiarity with carve-out plans and their requirements
- Their process for handling denied claims and appeals
- The reporting they provide and how often
- How they handle HIPAA compliance and data security
- References from mental health practices similar to yours
SwiftCare Billing specializes in mental health revenue cycle management. We work with therapy practices, group counseling centers, and psychiatric providers across the country. Our billing team handles verification, claim submission, denial management, and appeals — so your clinical staff can focus on patients instead of paperwork.
Frequently Asked Questions
What is the most common reason mental health claims get denied?
Missing or expired prior authorization is the leading cause of mental health claim denials. Many payers require approval before behavioral health services begin, and any gap in authorization coverage creates an immediate denial. After authorization issues, coding errors and insufficient documentation are the next most frequent causes.
How do I know if a patient needs prior authorization?
Ask during insurance verification. Call the provider line and ask specifically whether prior authorization is required for the service type and CPT codes you plan to bill. For new patients, ask about the initial evaluation and any ongoing therapy. Do not assume that the absence of a patient-reported authorization requirement means one is not needed.
Can I bill both a therapy session and a medication management visit in the same appointment?
Yes. When a prescribing clinician provides both an E/M service and psychotherapy in the same visit, both can be billed using the appropriate E/M code and the relevant psychotherapy add-on code (90833, 90836, or 90838). The documentation must clearly distinguish the time and content of each component of the visit.
What is the difference between 90834 and 90837?
The difference is session time. Code 90834 covers psychotherapy sessions that run 38 to 52 minutes. Code 90837 is for sessions of 53 minutes or more. The exact start and end time of the session must be documented in the clinical notes to support whichever code is billed.
How does telehealth affect mental health billing?
Telehealth mental health services are billed with the same CPT codes as in-person visits, but require the correct place of service code (02 or 10) and the appropriate telehealth modifier (GT or 95). Payer policies on telehealth vary significantly. Some cover it at the same rate as in-person visits; others apply different rules or reimbursement rates. Always verify telehealth coverage during benefits verification for each payer.
What happens if I submit a claim after the timely filing deadline?
Late claims are denied and in most cases cannot be recovered. The only exception is when the practice has documented proof that the delay was caused by the payer — for example, an insurer failed to process a corrected claim request within their own response window. Prevention is the only reliable solution. Build submission deadlines into your workflow and do not rely on end-of-month batch submissions.
How often should I verify insurance for ongoing patients?
Verify coverage at the start of each calendar year and any time a patient reports a change in insurance. Coverage can change due to an open enrollment switch, a job change, a spouse leaving an employer, or a lapse in premium payment. A patient who was covered last month may not be covered this month.
Is group therapy billed per session or per patient?
Group therapy (90853) is billed once per patient per session. If you see eight patients in a group, you submit eight separate claims, each for 90853. The code represents the service provided to each individual patient in the group context, not the group session as a whole.
What records do I need to keep for mental health billing compliance?
Keep clinical notes, treatment plans, authorization records, EOBs, and billing records for at least seven years. Some states require longer retention periods. Substance use disorder treatment records governed by 42 CFR Part 2 have their own retention and disclosure rules. Make sure your record storage complies with both HIPAA and any applicable state law.
Can SwiftCare Billing handle mental health billing for my practice?
Yes. SwiftCare Billing provides full-service mental health billing including eligibility verification, claim submission, denial management, payment posting, and appeals. We work with individual therapists, group practices, and psychiatric providers. Contact us at swiftcarebilling.com to learn how we can improve your revenue cycle.
Summary
Mental health claims submission is not forgiving of small mistakes. A missed authorization, an incorrect session duration code, or a documentation gap can mean weeks without payment on a claim that should have been processed on the first submission.
The practices that consistently get paid follow a disciplined process at every step: thorough verification before the first appointment, documentation that supports every code billed, clean claim submission with payer-specific rules accounted for, and prompt denial follow-up when claims are rejected.
If your practice is losing revenue to denials, experiencing long A/R cycles, or spending too much clinical staff time on billing administration, a billing partner with behavioral health expertise can change that outcome significantly.
SwiftCare Billing works with mental health practices across the country to improve clean claim rates, reduce denial backlogs, and bring more revenue in the door faster. Reach out at swiftcarebilling.com to learn more.